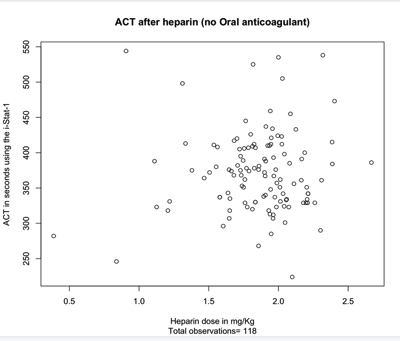
The amount of heparin to achieve a particular ACT is not easily calculated, due to the variable response to a known heparin concentration between patients.
In cardiac bypass procedures, a dose of 3mg (300 International Units or IU's) / Kg is often used. For catheter ablation for atrial fibrillation (CA-AF) procedures, 1 mg/Kg has been used historically. This approach is based on the erroneous assumption that every patient has the same response to a known concentration of heparin, based on weight. The volume of distribution does not correlate with weight alone.
If the patient is taking aspirin, warfarin or one of the newer oral anticoagulants such as Apixaban (Elequis), Dabigatran (Pradaxa), Rivaroxaban (Xarelto), Edoxaban, then a weight based protocol is inaccurate.
Even when on no oral anticoagulant, a weight based approach requires adjustment after the first dose.In a series of 513 patients undergoing CA-AF, where the desired ACT of between 300 and 400 was achieved, it was predicted from the population average heparin-ACT dose:response curve that a weight based dose of 1 mg/Kg would have failed to achieve an ACT of over 300. The minimum predicted ACT was 181 and the maximum predicted ACT was 233, with an average of 214.97
If the patients were having cardiac bypass surgery, the initial ACT after heparin would have been between 480 and 600 only 36.23% of the time.
The result of heparin administration to patients undergoing catheter ablation for atrial fibrillation are given below
Calculating the initial heparin dose